...Being Chronically Mommy!

...Being Chronically Mommy!
Baby Ticker
Blog with Integrity


Tuesday, May 2, 2017
Monday, April 3, 2017
I'm Not as Strong as Everyone Thinks I Am, Yet in My Journey I Will Become Strong!

It seems as though the popular phrase these days is "You are so strong." I
feel like I hear that all the time. I have to be honest, that phrase is making
me sick, people. Quit saying it! Ya know what? I'm actually not that strong!
I'm rather weak in the literal sense of the word. My physical therapist says
that I have weak muscles, weak joints, weak bones, weak tendons and
ligaments that attach the bones and muscles and joints, etc.
My hands and fingers are weak. I have a brace for my wrist, and a splint for
each finger. My knees are weak. I have a knee brace for both knees, and my
Avascular Necrosis is worse in both so I am just waiting for their collapse. My
ankles and feet are weak. I have to have ankle and arch supports, or achilles
tendinitis and plantar fasciitis ensue. Currently I have a hairline stress
fracture on top of my left foot from walking or standing. My spine is weak.
My hips were so weak that they have already collapsed and have already
been replaced. My shoulders and elbows are weak, leading to one shoulder
replacement thus far. I have had shingles 24 times! I'm on a 24 day course
of steroids right now for inflammation of a facial nerve from one of my
shingles outbreaks. On the steroids, my immune system was compromised
more, so now I am having yet another outbreak!
Why am I telling you this? I'm telling you this because I have several autoimmune and auto-inflammatory diseases. I wake up every morning just like everyone else does. The difference is that it takes me 30 minutes to get out of bed because I am so stiff and sore and achy and fatigued and just plain worn out to get my butt out of bed. I move very slowly for about 2 hours after finally maneuvering my crunchy self out of bed.
I take myself directly from my bed to the couch because it is too hard to do
much else. Once I take my 10-15 morning pills, I am capable of being a mom
to my 6 year old son Mick. I get his breakfast ready, his morning meds, help
with his clothes, and then we walk together to his school. I walk there and
back which is less than a mile. When I return home, I generally also return to the couch. I love the couch. I
set everything up around me that I will need for the day. I have my phone,
water, the TV remote, a snack, a book to read, something to work on, my
laptop, my pillow and a blanket.
I might have some errands to run or appointments to go to while he is at school. I might have some laundry to do. I might have to take Mick to dance class, soccer, baseball or choir after school. For the most part, I am on that couch all day except the walk to and from school and going to bed at night. I might decide to throw in a shower now and then when I get dirty too.
Now to my point...

I'm writing this because I am just so so so tired these days. Sure I do what I need to do for Mick and for my husband, but I am barely getting through the day here. My energy is at a zero. My tank is on empty. I have no extra stores. I have no idea what to do. I have tried resting all day, but it doesn't revive me. I have tried exercise, but it doesn't renew me.


If you are familiar with the Spoon Theory, I am out of spoons. I have no spoon reserves! I have not begged for, borrowed or stolen any spoons. I am just totally SOL! (I will accept donated spoons at any time however. Thanks in advance.)
I have had 10 surgeries, and never once was anyone here from my family
while I was in the hospital. Also, I have never had a visitor in the hospital
besides my own husband. I have had 3 joints replaced, 2 additional surgeries
on my shoulders, 2 additional surgeries on my hips, and my gallbladder
removed. I had 2 laparoscopic surgeries. I also have had 4 minor eye
procedures done. They are minor yes, but they still have to stick needles in
your eyeball. Your eyes are open so you see a needle coming straight at you!
It's horrifying! I had to drive myself with an infant after having tear duct
plugs placed, removed and tear ducts cauterized. The cauterization is painful
even with local anesthesia. They literally burn your tear ducts closed! It
smokes and BURNS, actually BURNS! I have had 2 epidural pain injections
and nerve blocks in my SI joints. I have had 2 endometrial biopsies in the
last two years. Do you know that they don't give you anesthesia for that?
They just cut pieces of your endometrial wall without any numbing or ice or
anything. I go every 4 weeks for an I.V. (Remicade) for my psoriatic arthritis. I always go alone and return by taxi home.

day, I remind myself to ask for help. Every single day, I remind myself that I can't do it alone. Every single day, I remind myself that I have gotten this far, and I can keep going. Every single day, I remind myself that, I may be weak right now, but if I play my cards right, I think I might come out with a good, strong hand.What's the secret? There really is no secret to being strong except figuring out that you had the answer all along. All of us who are weakened physically by chronic illnesses, somehow God has blessed us with a strong will, a strong heart and a strong soul. We have to figure that out on our own though. We have to get there on our own. For me, the realization comes every single day when I look at my son, and I understand that I am his STRONG Chronically Mommy! So...I may not be as strong as everyone thinks I am right now, but it is in my journey that I will become strong!

Friday, February 27, 2015
The World Has Stopped! Chronically Mommy Has The Flu!

So right now, I have the crud, the yuck, the blah, the flu!!! I get the flu shot every single year like the obedient chronic mommy that I am. This year Mick and I got ours together at his pediatrician office. My doctor informed me that it is only 23% effective this year. Great. Maybe I should look at it in a positive way, that I was the lucky one that got a flu shot and the flu...nah! This ain't lucky! I have been miserable. Mick was sick but only had a fever for maybe 12 hours at the longest. Then he had the coughing. He has asthma, so I made sure to use the nebulizer on him before taking him into the doctor. When I got him into the doctor, he said that I did fantastic! Great job Mommy!!! His lungs were great, no fever, no sign of flu complications and no infections. He is good. He has a small lingering cough, but it isn't worrisome.
As for me....well I started feeling sick last week on Thursday or Friday. I started Tamiflu on Sunday afternoon, and took the last pill today. I do feel better overall, but I am still coughing. I still have head congestion. I still feel so tired and fatigued. I still can't concentrate. The achiness is so much better than it was, thank goodness. It was horrible. I thought at first that I just had a cold and my autoimmune diseases were flaring causing severe pain everywhere. Well, come to find out that the flu causes severe aches and pains! It is no joke! Lemme tell ya!
I have made sure to get plenty of rest, plenty of fluids (water and OJ), and have been eating healthy foods. But I also have been eating whatever I will eat. I haven't been feeling like eating anything so if I have a taste for something, I eat it! I have been staying out of the cold air because it makes me cough and wheeze. I have been taking warm baths and showers. I like the showers to be steamier for my chest and sinuses.
I am amazed at how much Mommy is in control of and in charge of. When we are sick, it is clear that the house doesn't get clean, dinner doesn't get made, toys don't get put back where they belong, and important things don't get done! I think that for many of us, we don't look sick most of the time with our chronic illnesses, then when we get something acute like the flu, and we are down for the count, our significant other and our children, are really caught off guard. They are seriously surprised! My hubby asked me if I did the dark and light load of wash the other day. I was still in my P.J.s, and my hair was a greasy mess. I did nothing, absolutely nothing! I just sat on the couch and looked at the TV. I didn't even really watch TV. I just looked at the TV. That is when you know you are sick! Now the garbage disposal is broken, the water heater needs replaced, and my son flushed something down his toilet that has made it unable to flush or unclog. So the plumber has been here all day with me. Meanwhile, we have a weeks worth of dirty dishes piled on the countertop because of the garbage disposal, wall-to-wall hot wheel tracks because I haven't picked anything up, and laundry in piles in our bedroom because we had to get the water heater replaced today. The world has literally stopped around me! Nothing is happening! So I am writing my blog post. I figure I'm due.
Michael is 4 now. He is in pre-school at a Methodist church nearby. It's about 7 miles from our home. Of course with Atlanta traffic, it takes 30 minutes to get there and 30 minutes back. Nothing is ever easy! It is always so much harder when you are in pain, and then when you pile the flu bug on top of that...I have no words to describe it. I would suggest that you still get the flu shot. It still will guard against those particular strains. You never know which types will end up being the ones that go around, so better safe than sorry. My two cents.
I hope to talk to you all more often and soon!
Monday, May 6, 2013
“But you’re too young”

I fight very hard to spread awareness and educate those who are ignorant to what autoimmune arthritis is. When someone sees me park in a disabled parking spot and then tells me I can't park there because it is for someone who has a disability, I get very angry! I first think of it as a teachable moment. I tell the person that I have autoimmune arthritis. Of course, people never totally hear you! They many times will automatically come back with some kind of story about their grandmother having arthritis in her knee or something similar. Then they will end up somehow coming back to you, saying, "but you're too young..." Again, I will continue with the education. I will explain that autoimmune arthritis is not the same as your grandmother's arthritis. Then I will explain that even children can get autoimmune arthritis. Although, I am upset and mad that people don't know this, I try to use this as an opportunity to educate them and make them aware.
Because of many of my doctors' mentality of "but you're too young..." it took until I was 27 to finally have a name for my autoimmune arthritis disease. I was ignored, treated like a hypochondriac, and basically pushed away becaused of that mentality and by health professionals too! It isn't just uneducated, ignorant people who question whether or not I am too young to get arthritis. Doctors have also fallen into the category of people who need to be made aware of what autoimmune arthritis actually is and who it affects. It can be exhausting, overwhelming, and frustrating dealing with health care professionals who should know better, who should be keeping up with the current health diagnoses to know that even children get arthritis. It isn't just an old person's disease!
I look at it also from the angle that when I was very young, still a child, and I was trying to find out what was wrong with me, not one doctor tested me or looked into autoimmune arthritis diseases. When I was a child, there weren't many doctors that specialized in that area, especially for children, and very few doctors looked into a child having a type of arthritis because of the mentality of "but you're too young..." Although this has changed somewhat, and now there are pediatric rheumatologists to help diagnose young children earlier and without hitting a brick wall of "but you're too young." Of course, even though there are now pediatric rheumatologists, there are very few and not nearly enough to offer to those suffering from symptoms of autoimmune arthritis. If there were more pediatric rheumatologists, more children would be diagnosed sooner and more doctors would understand that with autoimmune arthritis there is no "too soon."
I know that when someone says to me or someone I know "but you're too young," that I get angry. I try to use that emotion toward gathering the information to teach those that are uneducated. There is no age on autoimmune arthritis disease. Everyone is different, and everyone is affected in different ways as well.
Saturday, April 13, 2013
April edition of the Patients for a Moment (PFAM) blog carnival--The Stresses of Chronic Pain--Misconceptions and Stigmas!

Misconception--n--a false or mistaken view, opinion, or attitude
Stigma--n--a distinguishing mark of social disgrace; a small scar or mark such as a birthmark; any mark on the skin, such as one characteristic of a specific disease; any sign of a mental deficiency or emotional upset
The most wide-spread misconception about chronic pain is that it results from a psychological disorder. Other misconceptions are that those with chronic pain should be able to tolerate their pain better as time goes on, that they are using pain to get narcotics, and that they exaggerate their pain to gain something like sympathy or money. There is a real catch 22 dilemma too. If they talk about their pain, they risk being labeled as hypochondriacs or fakers, and if they hide their pain, others will think their pain is insignigicant. It is so stressful that even the most stoic person will show signs of how taxing it is on a person. Chronic pain patients suffer daily from guilt, demoralization, and depression due to the negative perceptions of other people. You have probably heard the saying, "Pull yourself up by your bootstraps." For a chronic pain sufferer, you can't just talk yourself out of the pain. Then of course we have the patients who truly believe they must have sinned. They ask themselves everyday what they did wrong to endure chronic pain. Some call this "Job" Syndrome.
There is an overall agreement with patients of a generalized frustration about the public's perception of chronic pain. When the public tells you that you look fine so therefore you must be feeling fantastic, this says that pain is something that is worn on the outside when it really is something we wear on the inside. Men put more emphasis on how chronic pain affects their work, and women put more emphasis on how it affects their relationships. That makes sense though. Well, it does to me as a woman. I am worried if he will still love me like this, and he is worried if he can sit at his computer to complete his workday. Our coworkers, family and friends manifest their perceptions in so many ways, such as raising their eyebrows at you at work, a friend asking why you aren't feeling better yet when it has been a week, and even family members making the decision to turn their heads and minimize the problem. We have staggering statistics out there that one in three Americans suffes from chronic pain. Even with these statistics, there are societal biases in the workplace, restaurants, and even movie theaters. They are all designed for pain-free people!
People who suffer from chronic pain say that a huge factor behind the stigma is the invisible nature of most chronic pain, " You don't look like you're in pain." When people have easily visible proof of pain like swollen joints, canes, wheelchairs, braces, etc, they tend to report that the evidence of pain offers them validation in the eyes of others. If someone asked the question, "What does pain look like?" The answer is really more the visible evidence of the pain. You cannot actually see pain.
Stigma comes from the health care professionals, family, friends, the general public, the government, insurance companies, and even from chronic pain sufferers themselves. It can arise from within. Pain sufferers often experience guilt and therefore they blame themselves for their own pain. Health care professionals often present psychological obstacles for chronic pain patients. They believe the patient didn't follow the instructions, is receiving financial or some other secondary gain from receiving pain meds, or that the the patient is imagining the pain. Patients tend to go from one doctor to another to find relief with the burden being on the patient. Some doctors may focus too much on helping patients accept their pain and not enough on finding ways to help the pain. Why can't doctors work on treatment plans instead of telling patients they will have to just learn to live with the pain? This can lead to family members, especially spouses, feeling a sense of frustration that they can't do more to help the pain. Families tend to go from one extreme to the other, from gushing over the patient to acting angry even rejecting him. Many patients, especially as children will cope by hiding their pain. They fear rejection. Some parents will refer to the chronic pain as the "growing pains". People are afraid of people with chronic pain because they look so normal. They are afraid they could end up in the same scenario. They don't know how to act. They also fear they will "catch it".
"God I envy your life!" You hear this a lot because you may not have worked full time in the last two years. So many people just can't relate to what life would be like with chronic pain, and it just seems easier. Also, there are problems when you are job hunting. They may look at when you had those long periods of time where you didn't work. They will interpret that as a red, or warning, flag. You might be told that there is someone more qualified for the position than you. Chronic pain cannot be objectively validated like cancer, heart disease, or stroke. It can be more easily dismissed by employers and employees.
Inaccurate information about arthritis persists and is often spread. Such as:
- Arthritis is an old person's disease.
- Arthritis is induced by a cold, wet climate.
- Arthritis can be cured.
- Arthritis is caused by a poor diet.
- Arthritis consists of only minor aches and pains.
- "You felt fine yesterday....why so tired today?"
- "You have arthritis, you can't......"
- I Will Become Addicted
- I Will Run Out of Pain Relief Options if I Begin Treating Pain "Too Early"
- I Should Just Try to Stand the Pain
- Some of the Side Effects of Medication Are Just as Bad as the Pain
Friday, April 12, 2013
HAWMC Day 3 – Wordless Wednesday
HAWMC Day 3 – Wordless Wednesday

This picture symbolizes my conditions/diseases and my experiences as a person and mommy with joint diseases and as an advocate, an activist, a volunteer and a blogger!

Thursday, April 11, 2013
HAWMC Day 2 – Introductions
HAWMC Day 2 – Introductions

For day 2 of Health Activist Writer's Month Challenge, I am going to talk about what it is like to have a joint disease. There are 5 things you should know about my condition(s).
First, I have Psoriatic Arthritis with spinal involvement in my cervical spine, lumbar spine and SI joints. I have not been diagnosed with Ankylosing Spondylitis, but have been told by an orthopaedic spine surgeon that I most likely have a rare more severe form of Psoriatic Arthritis called Psoriatic Spondylitis. PsA is a chronic, inflammatory disease of the skin, scalp, nails and joint. The the psoriatic skin cell forms lesions. Second, 30% of people with psoriasis also develop inflammatory arthritis, which is PsA. The psoriasis precedes the arthritis in most of the people with PsA. The joints at the ends of the fingers are most commonly involved, but other joints can be involved too like the wrists, knees and ankles. Other symptoms that usually accompany it are in the fingernails and toes, and range from small pits in the nails to near total destruction of the nails, resembling nail fungus. Third, about 20% will end up with spinal involvement called Psoriatic Spondylitis. That inflammation in the spine can lead to complete fusion (Ankylosing Spondylitis) or only involve certain areas of the spine. When spinal involvement occurs, there is a greater chance of testing positive for HLA-B27, which is a genetic marker. Fourth, there is currently no known cure. There are treatments and medication only. Although the exact cause is unknown, heredity is thought to play a strong role. Up to 40% have a close relative with it. In identical twins, if one has it, the other has a 75% chance of also having it. Disease course and prognosis varies from person to person. The severity of the rash does not determine the severity of the arthritis. Also, the skin condition does not always occur at the same time as the arthritis symptoms.
Fifth, a number of medications can be used to help treat the symptoms of PsA: NSAIDs (non-steroidal anti-inflammatory drugs) to reduce the inflammation, joint pain and stiffness. DMARDs (disease-modifying anti-rheumatic drugs) are sometimes prescribed in more severe cases. All four of the TNF-a inhibitor medications approved by the FDA for ankylosing spondylitis are also approved for treating psoriatic arthritis. A dermatologist may also prescribe various medications to help treat the skin condition caused by the disease. Exercise is necessary. It helps keep the muscles strong to protect the joint. Not using a sore joint will cause the muscles to become weak and result in more pain. Other management tools include physical therapy, heat for stiffness, ice for swelling, physical therapy and surgery for those with severe joint damage. (Spondylitis Association of America http://www.spondylitis.org/)
Here are five more things you should know. First, I also have Avascular Necrosis (AVN). I was diagnosed in my hips, knees and shoulders. Also known as Osteonecrosis (ON), it affects about 20, new patients each year in the U.S. It mostly affects patients between 20 and 50 years old, with the average being in the late 30's. [Children from 2 to early teenage years get a form of ON called Legg-Calve-Perthes disease (Perthes for short) named after the three doctors who first described it. Treatment for Perthes is completely different than for adult ON.] It does not affect life expectancy so several hundred thousand patients are living with this disease in the U.S. To understand ON, you need to know that bone is a living tissue with cells and a blood supply. The word "osteonecrosis" means "death of bone", which occurs from the loss of the blood supply to the bone. Most people tend to use the term Avascular Necrosis, and AVN has become very popular in use because it's shorter to say and write. The risk of getting AVN is very small if the person is completely healthy, most likely less than one in 100,000. Most people who end up getting AVN likely have an underlying health condition. People that are over the age of 50 probably develop AVN from a fracture of the hip or very rarely from a disease of the major blood vessels of the lower leg. There are post-traumatic or non-traumatic forms of AVN.
Second, post-traumatic AVN is a common cause of AVN that includes displaced fractures or dislocations. Minor trauma or even most major injury does not often result in AVN. Certain fractures where blood vessels to part of the bone have been damaged may result in AVN. Non-traumatic AVN happens when there is no history of trauma. There are a number of risk factors. They do not know how these risk factors lead to the development of the disease, but they have different ideas. The ideas, however, have not yet been proven. There are some people who seem completely healthy with no detectable risk factors, and they consider the category "idiopathic" or "of unknown cause". Probably the most common cause of post-traumatic AVN of the hip and of other joints is a displaced fracture or a dislocation. The risk factors for AVN can be separated into definite and probably. The most common risk factor is a history of high dose steroid treatment for a medical condition such as RA or Lupus. Low dose steroid treatment is not thought to cause AVN. The next most common associated condition is a history of high alcohol use. The more alcohol you consume, the higher your risk of AVN.
| CAUSES OF OSTEONECROSIS | ||
DEFINITE
|
PROBABLE
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
| |
| ||
| ||
There is no known prevention. It is, however, believed to be true that if we eliminate or treat the risk factors, we can reduce the risk for getting AVN.
Third, 90% of people with AVN have it of the hip, however, it can also attack the knees, shoulders and ankles in that order. Nearly 3% will have multiple joints (3 or more) involved. We classify the joints the same, the disease progression is similar, passing from x-ray negative to x-ray positive without collapse to early collapse to extensive joint destruction. The knee can be divided into the medial compartment which is the inside of the knee between the femur and the tibia or shinbone, the lateral compartment which is the outside knee, and the patellofemoral compartment (kneecap). The most common involvement is the thigh bone portion of the knee. It is also not uncommon for the tibia or shinbone to also be involved. It is unusual for the patella (kneecap) to be involved. The natural progression of AVN in the knee is less certain than the hip. AVN of the shoulder has an even less certain natural history and natural progression than the knee. The area that is involved is the humeral head (shoulder) which is the area of the head which is in contact with the socket when the elbow is held at 40 degrees of flexion and 20 degrees away from the body. The ankle bone (talus) is not involved with AVN very often. It represents a real problem for both the physician and the patient.
Fourth, many patients with AVN have had it for a long time before they have any symptoms. The first symptoms are usually felt during an activity and are pain or aching in the joint that is affected. They usually begin slowly and may be sporadic at first. The pain may begin suddenly. With disease progression, the pain increases and is associated with stiffness and loss of motion of the joint that is involved. If the joint is in the leg, limping is common. The hip is the most common joint affected, and the AVN of the hip pain is usually felt in the groin. Stage I of the disease, x-rays appear normal, and an MRI is used to make the diagnosis. When it is seen on x-ray, it is not actually the dead bone that can be seen but the healing response of the living bone to the area of necrosis. The more advanced stages of AVN begin when the dead bone starts to fail mechanically through a process of microfractures of the bone. At some point, this results in damage to the other side of the joint, which requires major joint reconstruction. When more of the joint is damaged in the more advanced stages of AVN, it is less likely that you can preserve the natural joint. Joint replacements today are very successful even in the younger patients with AVN. The physician does prefer to preserve the normal joint when possible, but many do not see the doctor until the AVN is in the advanced stage of the disease.
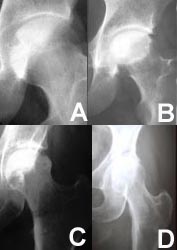 | These x-rays of the hip show the different stages of the disease. At first (stage I), there are no detectable changes on x-ray (fig A). In stage II, there are some changes but the surface is still intact (fig B). As the disease progresses, the surface begins to collapse (fig C) until, finally, the integrity of the joint is destroyed (fig D). |
The ball of the hip is called the femoral head and is the most frequent bone involved. It is rare for the entire weight-bearing surface of the femoral head to be involved, but if more than half of the surface is involved, treatments to preserve the ball have a much lower chance of success.
MRI's of Femoral Heads
diagnosed with Osteonecrosis | |
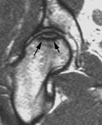 |  |
Small
Lesion |
Large
Lesion |
- X-ray
- Magnetic Resonance Imaging (MRI)
- Bone Scan
- Computed Tomography (CT)
- Biopsy
Fifth, crutches, canes or a walker help in alleviating pain with AVN. They can also protect the joint between the time of diagnosis and scheduling elective surgery. Limiting weight bearing may play a role in limiting progression while associated medical conditions are managed. Protected weight bearing alone is never an adequate treatment for AVN. It will not result in a cure of the condition no matter how long it is maintained. There are times when a patient has an associated medical condition that may result in being unable to have surgery. Protected weight bearing may be recommended for pain management. There aren't any drugs made for the prevention or treatment of AVN. To treat the disease, we have to understand how the disease develops first. Although there has been considerable effort by researchers, they cannot figure out what causes AVN when it is not the result of a fracture or dislocation. Even though the risk factors have been identified, it is not known if there would be an effect on the disease by eliminating or treating the risks. They are trying several different types of drugs:
- Lipid Lowering Medications
- Anticoagulants
- Hypertensive Medications
- Bisphosphonates

Here are five of my blog posts that I think are helpful to anyone with any joint disease or any chronic pain disease who are also mommies or newly diagnosed.
http://chronicallymommy.blogspot.com/2011_11_01_archive.html
http://chronicallymommy.blogspot.com/2012_04_01_archive.html
http://chronicallymommy.blogspot.com/2012/06/people-like-myself-can-raise-child.html
http://chronicallymommy.blogspot.com/2012_10_01_archive.html
http://chronicallymommy.blogspot.com/2013_01_01_archive.html
Here are three guest writers that I posted on my blog that I feel are helpful to anyone with any joint disease, chronic pain disease, and especially any autoimmune arthritis disease (more specifically JA) and the newly diagnosed.
What Do YOU Think of When You Hear The Word " ARTHRITIS"?--Ask Parker
http://chronicallymommy.blogspot.com/2012/07/what-do-you-think-of-when-you-hear-word.html
http://chronicallymommy.blogspot.com/2012/07/alexa-my-story.html
http://chronicallymommy.blogspot.com/2012/07/my-journey-with-jra.html
Chronically Mommy! 04/10 by Dana Morningstar | Blog Talk Radio
Chronically Mommy! 04/10 by Dana Morningstar | Blog Talk Radio
Chronically Mommy!
Let's talk frankly about what it's like to be a Mommy and to carry around the extra weight of Chronic Illnesses that include Chronic Pain, Disability, Autoimmune Arthritis Diseases, Avascular Necrosis, Fibromyalgia and more. Let's set the record straight about how we are not weak because of our Chronic Conditions, rather we are strong! We do both; we take care of a family as a Mommy and wake up and go to bed everyday questioning whether or not this is going to be a bad pain day or a better pain day. But mostly, we kiss boo-boos and wipe tears of the little ones in our lives so they don't have any pain. The conversation is worth your time! Share this!!!

{kind=link}
Listen to
internet radio with Dana Morningstar on Blog Talk Radio
Broadcast in Health
Monday, April 8, 2013
HAWMC Day 1 – Getting Started
HAWMC Day 1 – Getting Started

Welcome to our Third Annual Health Activist Writer’s Month Challenge!
My "Chronically Mommy" blog was my third blog in a series of three. I began writing about my spiritual journey in my first blog because when I became really sick, I became more spiritual and was searching for myself and my own path in this world. Then I began to write more about my experiences as a woman with chronic pain and awaiting my shoulder replacement surgery in my second blog. And in "Chronically Mommy", I became a mommy first and a woman with chronic pain and joint disease second. They go hand in hand however. I thought other mothers out there would like to know they are not alone. Also, we went through the adoption process, and it is a grueling process by itself, add the threatening shadows that seem to hover over the whole experience--chronic illness, disability and chronic pain--and you add additional stress, fear and concern that a birth mother will never choose you or that your "condition" will make it impossible to ever be matched with that one child that was meant to be yours. It was an extremely long and exhausting process, but we have a child and are the family we always wanted to be!
Every year I have wanted to get involved in HAWMC, but something has always gotten in the way--a shoulder replacement, a new baby or just the time it takes to be a mommy for a child in general, and a hip replacement. So I am a newbie to HAWMC! I have met so many people online since I began "Chronically Mommy" and have learned many tricks of the trade--being mommy and chronic!
I have always had a diary and a journal. Blogging has become just another way to journal for me. I like it better though because people can respond and make comments. When you write in your own journal, you have no criticism. If I ask a question, I get answers--sometimes many, many answers. If I learn something new and want to pass it on, I can blog about it, and I have then educated and spread awareness. And nowadays, I can press one button and the blog post link goes to multiple sites at once, like Facebook, LinkedIn and Twitter so the information is even more widespread than when I first began!
I write about health topics as a Mommy because it is something that I know, that I experience and that I have the ability to share with others. I am an advocate. I am an activist. I want to share with the world what I know about being a Mom with chronic pain, disability, chronic illness, autoimmune arthritis, and other conditions. Even if someone reads my blog that doesn't have exactly the same diseases or conditions, I feel that I am able to reach anyone who shares a chronic illness, chronic pain or disabling condition. That is really the most important thing to me, to reach as many Chronic Mommies as I possibly can to help them to be, feel and live as well as possible!



Subscribe to:
Posts (Atom)