


HAWMC Day 2 – Introductions

For day 2 of Health Activist Writer's Month Challenge, I am going to talk about what it is like to have a joint disease. There are 5 things you should know about my condition(s).
First, I have Psoriatic Arthritis with spinal involvement in my cervical spine, lumbar spine and SI joints. I have not been diagnosed with Ankylosing Spondylitis, but have been told by an orthopaedic spine surgeon that I most likely have a rare more severe form of Psoriatic Arthritis called Psoriatic Spondylitis. PsA is a chronic, inflammatory disease of the skin, scalp, nails and joint. The the psoriatic skin cell forms lesions. Second, 30% of people with psoriasis also develop inflammatory arthritis, which is PsA. The psoriasis precedes the arthritis in most of the people with PsA. The joints at the ends of the fingers are most commonly involved, but other joints can be involved too like the wrists, knees and ankles. Other symptoms that usually accompany it are in the fingernails and toes, and range from small pits in the nails to near total destruction of the nails, resembling nail fungus. Third, about 20% will end up with spinal involvement called Psoriatic Spondylitis. That inflammation in the spine can lead to complete fusion (Ankylosing Spondylitis) or only involve certain areas of the spine. When spinal involvement occurs, there is a greater chance of testing positive for HLA-B27, which is a genetic marker. Fourth, there is currently no known cure. There are treatments and medication only. Although the exact cause is unknown, heredity is thought to play a strong role. Up to 40% have a close relative with it. In identical twins, if one has it, the other has a 75% chance of also having it. Disease course and prognosis varies from person to person. The severity of the rash does not determine the severity of the arthritis. Also, the skin condition does not always occur at the same time as the arthritis symptoms.
Fifth, a number of medications can be used to help treat the symptoms of PsA: NSAIDs (non-steroidal anti-inflammatory drugs) to reduce the inflammation, joint pain and stiffness. DMARDs (disease-modifying anti-rheumatic drugs) are sometimes prescribed in more severe cases. All four of the TNF-a inhibitor medications approved by the FDA for ankylosing spondylitis are also approved for treating psoriatic arthritis. A dermatologist may also prescribe various medications to help treat the skin condition caused by the disease. Exercise is necessary. It helps keep the muscles strong to protect the joint. Not using a sore joint will cause the muscles to become weak and result in more pain. Other management tools include physical therapy, heat for stiffness, ice for swelling, physical therapy and surgery for those with severe joint damage. (Spondylitis Association of America http://www.spondylitis.org/)
Here are five more things you should know. First, I also have Avascular Necrosis (AVN). I was diagnosed in my hips, knees and shoulders. Also known as Osteonecrosis (ON), it affects about 20, new patients each year in the U.S. It mostly affects patients between 20 and 50 years old, with the average being in the late 30's. [Children from 2 to early teenage years get a form of ON called Legg-Calve-Perthes disease (Perthes for short) named after the three doctors who first described it. Treatment for Perthes is completely different than for adult ON.] It does not affect life expectancy so several hundred thousand patients are living with this disease in the U.S. To understand ON, you need to know that bone is a living tissue with cells and a blood supply. The word "osteonecrosis" means "death of bone", which occurs from the loss of the blood supply to the bone. Most people tend to use the term Avascular Necrosis, and AVN has become very popular in use because it's shorter to say and write. The risk of getting AVN is very small if the person is completely healthy, most likely less than one in 100,000. Most people who end up getting AVN likely have an underlying health condition. People that are over the age of 50 probably develop AVN from a fracture of the hip or very rarely from a disease of the major blood vessels of the lower leg. There are post-traumatic or non-traumatic forms of AVN.
Second, post-traumatic AVN is a common cause of AVN that includes displaced fractures or dislocations. Minor trauma or even most major injury does not often result in AVN. Certain fractures where blood vessels to part of the bone have been damaged may result in AVN. Non-traumatic AVN happens when there is no history of trauma. There are a number of risk factors. They do not know how these risk factors lead to the development of the disease, but they have different ideas. The ideas, however, have not yet been proven. There are some people who seem completely healthy with no detectable risk factors, and they consider the category "idiopathic" or "of unknown cause". Probably the most common cause of post-traumatic AVN of the hip and of other joints is a displaced fracture or a dislocation. The risk factors for AVN can be separated into definite and probably. The most common risk factor is a history of high dose steroid treatment for a medical condition such as RA or Lupus. Low dose steroid treatment is not thought to cause AVN. The next most common associated condition is a history of high alcohol use. The more alcohol you consume, the higher your risk of AVN.
| CAUSES OF OSTEONECROSIS | ||
DEFINITE
|
PROBABLE
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
| |
| ||
| ||
There is no known prevention. It is, however, believed to be true that if we eliminate or treat the risk factors, we can reduce the risk for getting AVN.
Third, 90% of people with AVN have it of the hip, however, it can also attack the knees, shoulders and ankles in that order. Nearly 3% will have multiple joints (3 or more) involved. We classify the joints the same, the disease progression is similar, passing from x-ray negative to x-ray positive without collapse to early collapse to extensive joint destruction. The knee can be divided into the medial compartment which is the inside of the knee between the femur and the tibia or shinbone, the lateral compartment which is the outside knee, and the patellofemoral compartment (kneecap). The most common involvement is the thigh bone portion of the knee. It is also not uncommon for the tibia or shinbone to also be involved. It is unusual for the patella (kneecap) to be involved. The natural progression of AVN in the knee is less certain than the hip. AVN of the shoulder has an even less certain natural history and natural progression than the knee. The area that is involved is the humeral head (shoulder) which is the area of the head which is in contact with the socket when the elbow is held at 40 degrees of flexion and 20 degrees away from the body. The ankle bone (talus) is not involved with AVN very often. It represents a real problem for both the physician and the patient.
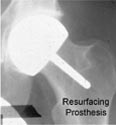
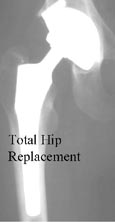
Fourth, many patients with AVN have had it for a long time before they have any symptoms. The first symptoms are usually felt during an activity and are pain or aching in the joint that is affected. They usually begin slowly and may be sporadic at first. The pain may begin suddenly. With disease progression, the pain increases and is associated with stiffness and loss of motion of the joint that is involved. If the joint is in the leg, limping is common. The hip is the most common joint affected, and the AVN of the hip pain is usually felt in the groin. Stage I of the disease, x-rays appear normal, and an MRI is used to make the diagnosis. When it is seen on x-ray, it is not actually the dead bone that can be seen but the healing response of the living bone to the area of necrosis. The more advanced stages of AVN begin when the dead bone starts to fail mechanically through a process of microfractures of the bone. At some point, this results in damage to the other side of the joint, which requires major joint reconstruction. When more of the joint is damaged in the more advanced stages of AVN, it is less likely that you can preserve the natural joint. Joint replacements today are very successful even in the younger patients with AVN. The physician does prefer to preserve the normal joint when possible, but many do not see the doctor until the AVN is in the advanced stage of the disease.
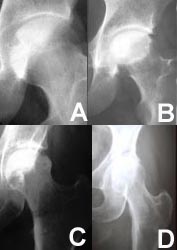 | These x-rays of the hip show the different stages of the disease. At first (stage I), there are no detectable changes on x-ray (fig A). In stage II, there are some changes but the surface is still intact (fig B). As the disease progresses, the surface begins to collapse (fig C) until, finally, the integrity of the joint is destroyed (fig D). |
The ball of the hip is called the femoral head and is the most frequent bone involved. It is rare for the entire weight-bearing surface of the femoral head to be involved, but if more than half of the surface is involved, treatments to preserve the ball have a much lower chance of success.
MRI's of Femoral Heads
diagnosed with Osteonecrosis | |
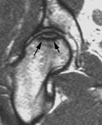 |  |
Small
Lesion |
Large
Lesion |
- X-ray
- Magnetic Resonance Imaging (MRI)
- Bone Scan
- Computed Tomography (CT)
- Biopsy
Fifth, crutches, canes or a walker help in alleviating pain with AVN. They can also protect the joint between the time of diagnosis and scheduling elective surgery. Limiting weight bearing may play a role in limiting progression while associated medical conditions are managed. Protected weight bearing alone is never an adequate treatment for AVN. It will not result in a cure of the condition no matter how long it is maintained. There are times when a patient has an associated medical condition that may result in being unable to have surgery. Protected weight bearing may be recommended for pain management. There aren't any drugs made for the prevention or treatment of AVN. To treat the disease, we have to understand how the disease develops first. Although there has been considerable effort by researchers, they cannot figure out what causes AVN when it is not the result of a fracture or dislocation. Even though the risk factors have been identified, it is not known if there would be an effect on the disease by eliminating or treating the risks. They are trying several different types of drugs:
- Lipid Lowering Medications
- Anticoagulants
- Hypertensive Medications
- Bisphosphonates

Here are five of my blog posts that I think are helpful to anyone with any joint disease or any chronic pain disease who are also mommies or newly diagnosed.
http://chronicallymommy.blogspot.com/2011_11_01_archive.html
http://chronicallymommy.blogspot.com/2012_04_01_archive.html
http://chronicallymommy.blogspot.com/2012/06/people-like-myself-can-raise-child.html
http://chronicallymommy.blogspot.com/2012_10_01_archive.html
http://chronicallymommy.blogspot.com/2013_01_01_archive.html
Here are three guest writers that I posted on my blog that I feel are helpful to anyone with any joint disease, chronic pain disease, and especially any autoimmune arthritis disease (more specifically JA) and the newly diagnosed.
What Do YOU Think of When You Hear The Word " ARTHRITIS"?--Ask Parker
http://chronicallymommy.blogspot.com/2012/07/what-do-you-think-of-when-you-hear-word.html
http://chronicallymommy.blogspot.com/2012/07/alexa-my-story.html
http://chronicallymommy.blogspot.com/2012/07/my-journey-with-jra.html
1 comment:
As a sign of gratitude for how my son was saved from fibromyalgia , i decided to reach out to those still suffering from this.
My son suffered fibromyalgia in the year 2013 and it was really tough and heartbreaking for me because he was my all and the symptoms were terrible, he always complain of joint stiffness, and he always have difficulty falling asleep . we tried various therapies prescribed by our neurologist but none could cure him. I searched for a cure and i saw a testimony by someone who was cured and so many other with similar body problem, and they left the contact of this doctor who had the cure to fibromyalgia . I never imagined fibromyalgia has a natural cure not until i contacted him and he assured me my son will be fine. I got the herbal medication he recommended and my son used it and in one months time he was fully okay even up till this moment he is so full of life. fibromyalgia has a cure and it is a herbal cure contact the doctor for more info on drwilliams098675@gmail.com on how to get the medication. Thanks for reading my testimony.
Post a Comment